- COMSOL News 2025
- COMSOL News Special Edition: Food Industry
- COMSOL News 2023
- COMSOL News 2022
- COMSOL News 2021
Simulation App Introduces Personalized Oncology Care
To predict tumor progression for breast cancer, a spin-off company called initiatives for Bio-Materials Behavior (iBMB Srls) in Potenza, Italy, developed a simulation application to help healthcare professionals better monitor tumor lesion volumes and treatment effectiveness prior to neoadjuvant chemotherapy.
By Dixita Patel
September 2024
Worldwide, one of the most common types of cancer among women is breast cancer, and while there have been improvements to the current available cancer treatments, determining an accurate prognosis for breast cancer remains a challenge. One approach that could help improve patient care is predictive oncology. This approach is a shift from traditional cancer treatments (Figure 1), instead taking patient-specific data into account in a more precise and personalized way so that oncologists can better understand how tumors will respond to specific treatments.

When combined with computational modeling (Figure 2), predictive oncology can be used to anticipate treatment outcomes for patients using algorithms and machine learning techniques. For instance, mathematical equations that describe the biological and physical mechanisms behind cancer growth, as well as treatment responses, can be used to create deterministic models of tumor progression. (Ref. 1) One company that is using mathematical equations in this way is initiatives for Bio-Materials Behavior (iBMB Srls), a spin-off of the University of Basilicata. iBMB Srls used the COMSOL Multiphysics® software to create CancerMate, a simulation app that is based on a mathematical model that represents tumor behavior. Oncologists can use the app to better monitor and assess solid tumor progression for breast cancer, specifically nonmetastatic triple-negative breast cancer, treated with neoadjuvant LYNPARZA® therapy. With the results from the app, oncologists can adjust therapeutic strategies accordingly to help optimize therapy effectiveness and minimize adverse effects.
"The current treatments on the market lack personalization and precision," said Gianpaolo Ruocco, CEO of iBMB Srls. "CancerMate allows doctors to run virtual scenarios, reducing the burden on the patient and the cost of the treatment."
Determining Tumor Volume via Virtual Biomarkers
The intended focus of the CancerMate app is to quantify lesion volumes before a patient undergoes neoadjuvant chemotherapy to reduce tumor size. The Mark 1 version of CancerMate was validated against clinical data of patients with nonmetastatic triple-negative breast cancer, treated with the drug LYNPARZA® (olaparib). (Ref. 2) The clinical experiment involved a retrospective cohort of 17 patients, and the data from the experiment was used to test an in silico reactive-diffusive model (based on partial differential equations, or PDEs) to predict the metabolic response of breast cancer, virtualize tumor progression, and predict tumor dynamics in response to therapy for individual patients.
The clinical experiment helped the team identify key breast carcinoma biomarkers, which are necessary for predicting how a tumor will respond to treatment. In a clinical setting, biomarkers are indicators of a patient's health measured from bodily fluid, such as blood, and tissue tests. During the study, tumor-infiltrating lymphocytes (TILs), which describe immune response, and protein Ki67, which describes tumor aggressiveness, were closely monitored over time. In the CancerMate app, virtual biomarkers are integrated into models as digital or computational indicators that represent biological processes or disease characteristics, intended to supplement or predict traditional clinical biomarkers (Ref. 2).
For the clinical experiment, the mathematical model incorporated the biomarkers for personalized malignancy (rc) and personalized pharmacodynamic efficiency (ϵPD), which correlate to the traditional biomarkers Ki67 and TILs. The biomarkers helped to quantify the effectiveness of olaparib during the experiment. As explained in a research paper relating to the clinical experiment, "The model showed, without any preliminary assumption, the effective pharmacodynamic efficiency of olaparib was strongly dependent on basal TILs level and metric tumor volume V or metabolic tumor volume SUVmax growth rate. V or SUVmax were represented by a mathematical parameter that in our case was directly dependent on Ki67 expression and TILs count." (Ref. 3)
To illustrate the mathematical model and visually compare the predicted and observed values from the experiment, the team at iBMB used a Gompertzian curve to model tumor growth, specifically during the phases before and after the administration of olaparib (Figure 3). The curve represents metric tumor volume V over time (t) over three different cancer growth phases. These three phases are free proliferation, challenged proliferation, and uncontrolled growth (denoted as "Phase I", "Phase II", and "Phase III", respectively, in Figure 3).
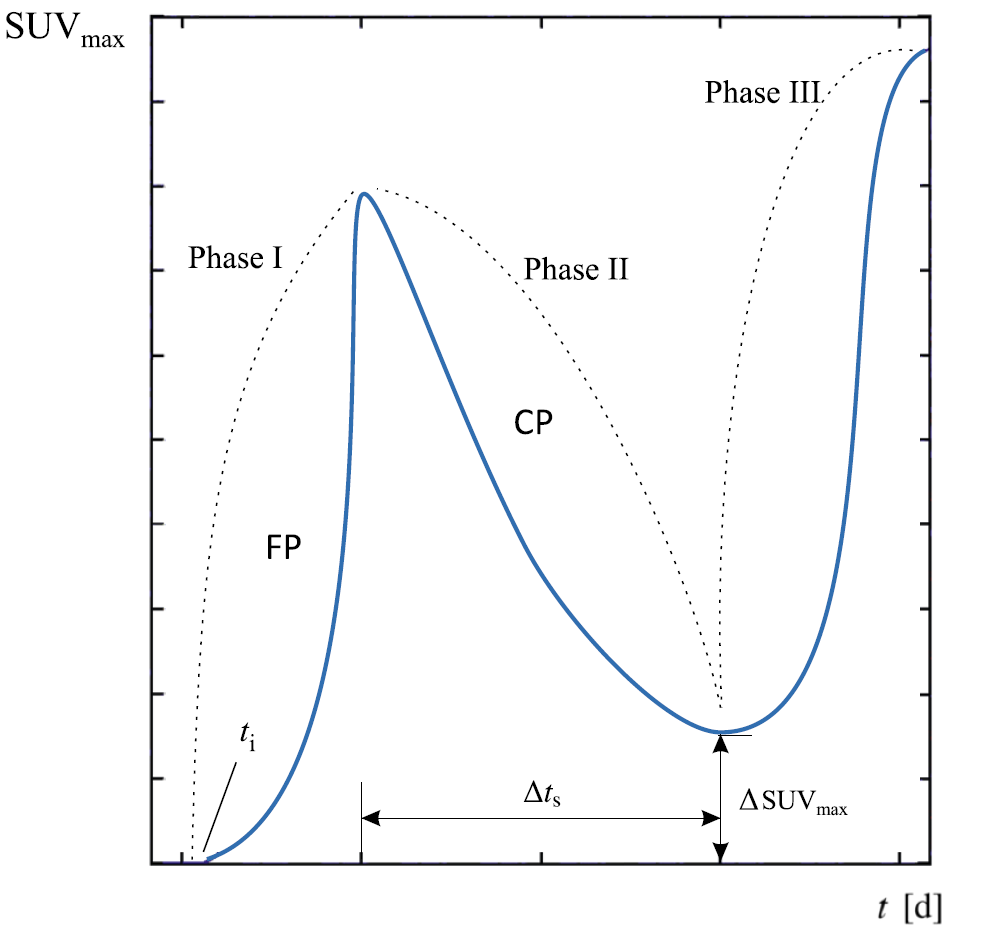
Phase I (free proliferation), begins at an unknown starting point (ti) and continues until the diagnosis for the tumor is made (t = 0). At this point, a diagnostic image is performed and an oncologist will determine which therapy the patient needs. Following this, Phase II (challenged proliferation) represents the start of therapy and observes the partial regression of the tumor due to therapeutic intervention. Lastly, Phase III (uncontrolled growth) is an observation period to see if there is further tumor growth or an increase in metabolic activity after treatment has ended or resistance develops. This phase helps to highlight if further monitoring and additional treatments are needed. The validated mathematical model was integrated into CancerMate, where rc and ϵPD are the two primary virtual biomarkers.
CancerMate: A Leap Toward Personalized Oncology
Ruocco and the team developed CancerMate using the equation-based modeling functionality in COMSOL Multiphysics. They integrated the PDEs (based on transport phenomena) that represent tumor growth and therapy responses and thus could be used to simulate the proliferation of cancer cells and the effects of neoadjuvant chemotherapy. The app was created with the Application Builder in COMSOL Multiphysics and turned into a standalone app with COMSOL Compiler™, an add-on product for compiling apps with the click of a button (Figure 4). By converting CancerMate into a standalone app, Ruocco is able to easily distribute the app to clinicians, enabling them to perform virtual scenarios and receive detailed information about cancer progression directly at their desktop.
The interface of the app includes the ability to input patient data, display numerical results, and visualize the graphical progress of predicted lesion volume and integrated drug concentration over time (Figure 5). The input fields for the patient-specific biomarkers are the starting points for the oncological predictions, where the first input field is an estimation of the start time of the tumor lesion. The other input fields include the total observation period (which depends on the therapy that will be used), patient mass, body surface area, and the baseline Ki67 and TILs values. Additionally, input fields for the dosage and baseline creatinine indicators are included, which directly relate to the pharmacodynamics (how the drug fights the tumor) and the pharmacokinetics (how the body disposes the drug by bodily functions).
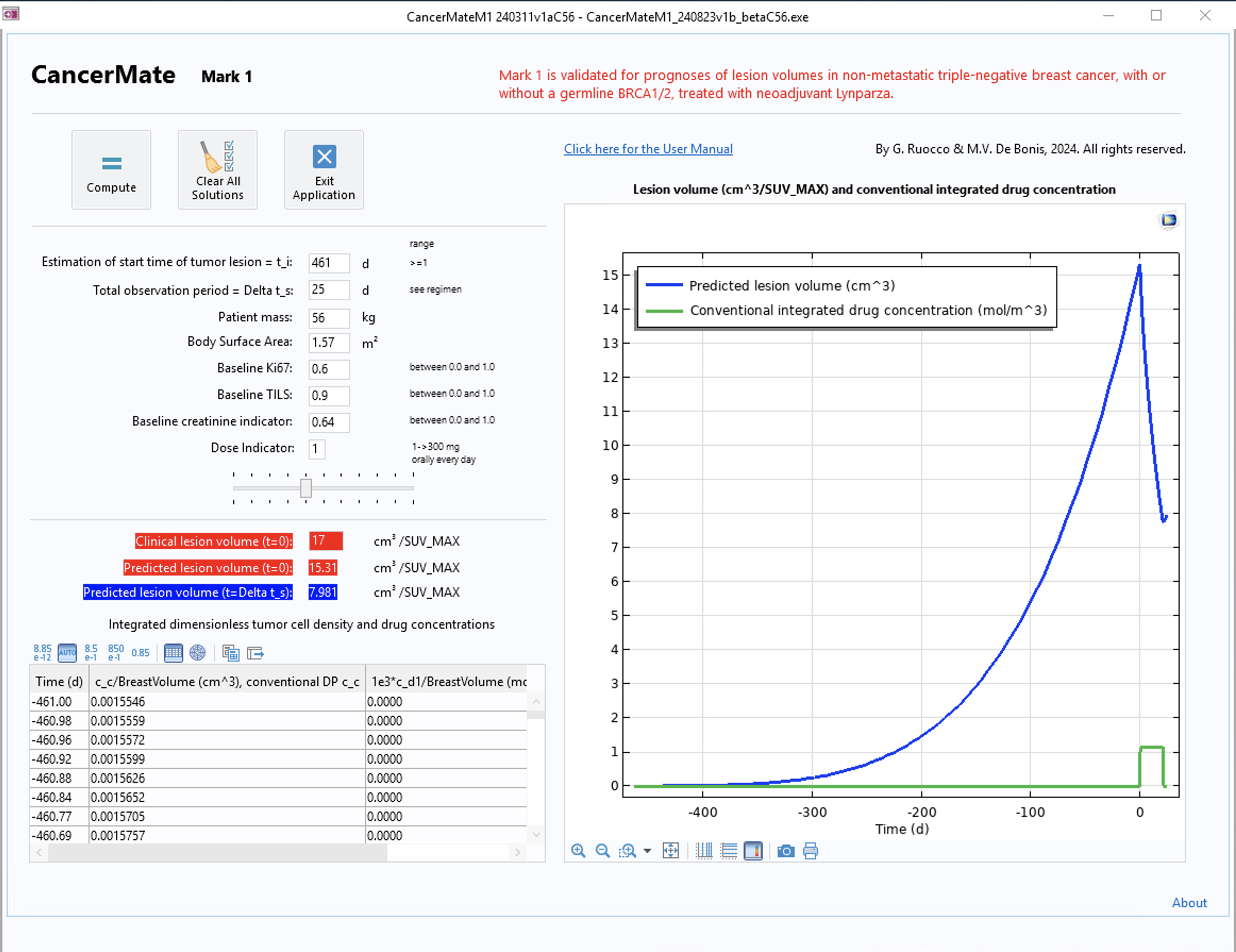
The app uses the mathematical model to integrate clinical data that includes baseline measurements such as SUVmax, TILs, and Ki67. The virtual biomarkers, rc and εPD, inform the model's predictions, and then the app will apply these biomarkers to a set of equations that describe tumor growth and response to treatment over time. After computing, the numerical results for the predicted clinical lesion values at t = 0 and t = Δts are displayed, and a graphic shows the progress of the predicted cancer lesion volume and the integrated drug concentration. By utilizing the built-in functionality in COMSOL Multiphysics for solving complex PDEs, CancerMate provides clinicians with an efficient way to monitor a patient’s response to therapy.
The Future of CancerMate and Virtual Human Twins in Oncology
CancerMate's user-friendliness and simulation capabilities make it valuable in personalized cancer treatment for oncologists and pharmaceutical researchers. The current version of CancerMate is ready for implementation in a clinical setting, specifically for the treatment of triple-negative breast cancer and LYNPARZA® therapy. Ruocco said that upon further dataset availability, the underlying model could be trained to cover more couplings between different breast cancer subtypes and therapies. Moreover, while the app is currently focused on breast cancer, the team at iBMB plans to extend the underlying technology of the app to also focus on other types of cancer and drug products.
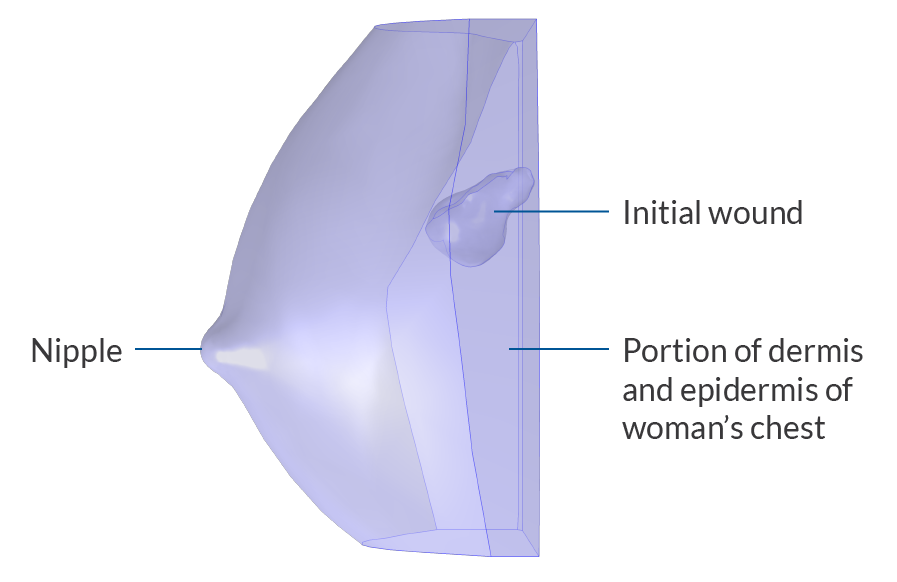
In addition to extending the use of the app, iBMB intends to promote CancerMate as a tool that can be used alongside technology for creating virtual human twins (VHTs), with the intent of creating twins that represent a cancerous disease state. VHTs are significant because they have the potential to improve precision and advance customized cancer care. Ruocco said that one possibility for VHTs is to project them via a head-mounted display that surgeons could wear (Figure 6). With such a headset, the surgeon would be immersed in a virtual reality where they could see, for instance, if a lesion in a breast was too close to the bone and, depending on the results, adjust treatment plans as needed. "[VHTs are] a way of approaching medicine in a personalized and precise way, which is a change of paradigms," said Ruocco.

As predictive oncology evolves, tools like CancerMate can shape personalized medicine by helping clinicians assess and monitor tumor lesion volumes. As explained by Ruocco, "Patients are often treated longer than necessary, but this can be modified with in silico tools."
References
- CFDNOVA, Google Sites; https://cfdnova.unibas.it
- G. Ruocco, User Manual for CancerMate — Mark 1, Apr. 2024.
- F. Schettini et al., "Computational Reactive–Diffusive Modeling for Stratification and Prognosis Determination of Patients with Breast Cancer Receiving Olaparib," Scientific Reports, July 2023; https://doi.org/10.1038/s41598-023-38760-z
LYNPARZA is a registered trademark of AstraZeneca AB.